



Neck & Upper Back Pain
Carpal Tunnel Syndrome (CTS) & Prehension
What is CTS...and should I be worried?
A good story, like the one I'm about to share about carpal tunnel syndrome, needs a lot of setup. It gets the boring stuff out of the way so there can be more action later, so bear with me please!
Carpal tunnel syndrome (CTS) affects the hand with numbness, tingling, or a weakening of the muscles. As for the carpal tunnel itself, that part is a space in your wrist, bordered by the transverse carpal ligament and a few bones, where a couple of muscle tendons and the median nerve passes through (more on this later). If this space gets smaller or narrower, pressure builds up on this median nerve, which leads to the decreased sensation and muscle weakness. Changes in muscles strength can have a larger impact than you might expect, as a lot of tasks in our lives depend on fine motor control and grasp. For example something simple like writing would be incredibly hard with impairment of grip between your thumb and fingers. Even typing would be difficult with weakened hand muscles, especially if there is a lack of sensory feedback. Exactly which parts of the hand are in trouble with CTS? We'll get into that below.
So who should be worried about CTS? A review of literature from Palmer, Harris, and Coggon (2007) found a number of work related risks that increase the chance of developing CTS. One of the major risk factors is employment in a field which requires the use of hand-held vibratory tools, such as construction work. Repetitive movements which require wrist bending (a lot of office work may require this) will also increase the chance of developing CTS. However, a YouTube video by Dr. Terry Zachary (2008) suggested that it is actually an imbalance between the muscles that control wrist flexion and extension which lead to the development of CTS and highlighted the importance of bending the wrist forward and back to exercise it. As a lot of functional tasks like getting dressed or brushing your teeth require the wrist to be in a flexed state, there may be some basis to this theory on the importance of balance. The video and a short critique of its information can be found on the critiques page, listed above.
For a while now, there has been an association of computer work with CTS, however this correlation may not be backed by research. The review by Palmer, et al. (2007) included articles on keyboard and computer work and was inconclusive on their affect on developing CTS. Another review by Thomsen, Gerr, and Atroshi (2008) look specifically at CTS and mouse and keyboard work, which again found that there was insufficient evidence to support any causation. In fact, Scott Aronin (2011), a Certified Strength and Conditioning Specialist, points out on his site (found on the critiques page) that the median nerve, like all nerves, has its roots in the spine. Therefore, issues with the neck and shoulder blade, which our site describes extensively, can also impinge on the median nerve to affect its function. This would probably cause more issues than just carpal tunnel syndrome, but the role of neck and back pain in CTS is something to consider.
However, there has been research to show a correlation between computer and keyboard work to increased pressure in the carpal tunnel, though it is unclear if this increased pressure necessarily leads to the development of CTS (Keir, Bach, & Rempel, 1999). However, researchers Ben Goss and Dr. John Agee (2011) suggest that pressure in the carpal tunnel, especially during grip and pinch tasks, is necessary to keep the ligament that borders the carpal tunnel loose and keep resting pressure lower. Therefore, our story with CTS is a little more complicated than we might've imagined.
The major players
Information from Allman, 2015a; Allman, 2015b
So what's all this median nerve, carpal tunnel business that's giving me all this trouble? The GIF to the right gives a pretty good general overview, complete with a surgical solution, if you just want to skip ahead to the big reveal.
Still with me? Great! We'll try and make this anatomy crash course as quick and painless as possible. The first thing you need to know about is the median nerve. It's actually the good guy here, trying to mind its own business and do its job. It starts up near the armpit and runs down along the arm, innervating (connecting to) muscles in the forearm along the way so it can send them signals and activate them when you need to use them. These forearm muscles are important for prehension (Pre...what? Spoilers below), but not so much for CTS. Why? Because the median nerve can do its job just fine until it gets to the big, bad carpal tunnel, it's the real villain here (not really, but it makes things more interesting).
Hand and Upper Limb Clinic, 2010

Dun dun dun....here it is, the big reveal, the infamous carpal tunnel! Bit anticlimactic you say? I mean it's no Keyser Soze but this is definitely more important to know than some made up crime genius. So anyways, the picture to the left shows you the carpal tunnel, made up by the Transverse carpal ligament and the Carpal bones. Unfortunately, to get to its final destination in the hand, the median nerve has to pass through the tunnel which is crowded up by a bunch of tendons from those forearm muscles mentioned earlier (bet you didn't see that twist coming). So basically the problem arises when the tunnel gets too cramped (through things like swelling in the wrist) and the our friend the median nerve gets pinched, which stops its functioning for everything downstream of the tunnel (ie. all its functions in the hand).
Carpal tunnel syndrome picture
Prehension...what's that?
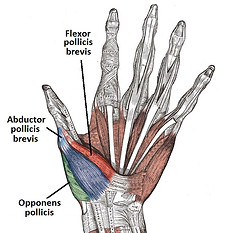
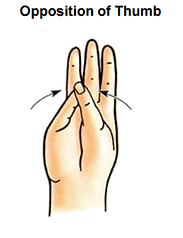
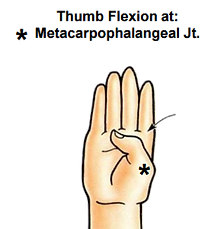
So who does this affect the most? The poor little thumb. It's kind of like an action movie where the hero makes the bad guy angry so the bad guy goes after the hero's children, such a tragedy. To get into the nitty-grittiness of it, the part that the median nerve innervates in the hand is the thenar eminence (meaty part of the thumb, lovely group picture of them below), which is comprised of three muscles: the abductor pollicis, the flexor pollicis brevis, and the opponens pollicis. As the names imply (or not, they're pretty confusing names), the muscles are responsible for abducting, flexing, and opposing the thumb. Words aren't the best for describing these actions, so take a look at the pictures below! The median nerve also helps to control the lumbricals (another group of muscles) that go to the index and middle finger. These lumbricals are responsible for flexing these fingers at the knuckles while keeping them extended the rest of the way, as seen below. All these muscles can play a large part in everyday hand use, especially grip and hand dexterity, but more on that later.



The other crucial job for the median nerve in the hand is its sensory component. The median nerve branches off and sends some representatives to collect sensory information from the half of your hand closer to the thumb on the palm side, and the upper halves of the index and middle fingers on the back of the hand (seen in the blue and outlined in the red boxes below). This is what contributes to the numbness or tingling in the hands for CTS because the median nerve can't do its sensory job in retreiving the sensory inputs from these parts of the hand. Keep this in mind as you read on...
Thenar eminence picture from TeacMenatomy.
Other images: Ballman, 2015b
Information from Spaulding, 1988
So I've mentioned this prehension thing a few times now and like every good story, it needs some character development. In a very basic sense, prehension is the grasping movement you perform with your hand. But prehension isn't just a simple one-dimensional character, it has a lot of different characteristics to it. For example...

Force: Technically, a force is an interaction that will cause movement when it is applied to an object and there isn't another force to cancel it out. So if I'm pulling a beloved object towards me and my arch nemesis is pulling it away from me with the same amount of force (pictured to the right), it would stay stationary because the forces are equal in magnitude and opposite in direction. For prehension's sake, we can consider the force as the strength of your grip, either through each individual finger or as a whole.
Torque: So remember when I said that forces applied on an object equal in magnitude but opposite in direction would cause the object to be stationary? Well that's because I forgot about torque. Torque is a force that causes an object to undergo rotational movement, spinning about an axis. So the object can still stay in place, as in it won't move anywhere, but it'll be spinning. For example when you're spinning a coin, you would stand it upright, push one edge of the coin down and push the other edge up. Even if these two pushes were equal in force, the coin would still spin because you applied them at different places on the coin and create a non-zero rotational force. When this non-zero rotational force exists, it's referred to as a moment (not the romantic, touching type, this isn't that kind of story). Generally, you want to avoid creating moments while grasping, as this causes the object to spin.

Children fighting over toys
Spinning quarter
Friction: Lastly, we'll briefly talk about friction (even though there's been a lot of friction between our characters throughout). Friction exists anytime two objects are in contact and one attempts to move in relation to the other. Friction is the force that works to resist this motion. For example, when you're walking, there's friction between your shoes and the floor as you push off. If there was no friction (like if you were walking on ice), your foot would just continue going backwards and you'd fall flat on your face! In prehension, friction is very important in keeping an object within your grasp. When you're picking an object up with a cylindrical grip (seen below), the friction between your hand and the object plays a large role in keeping it from slipping through your hand. An interesting thing to note is that the greater the perpindicular (in relation to the direction of movement) force is, the greater the frictional force will be!
For a more a more detailed overview of these terms and more, check out this little side-plot here.
The thing about prehension though is that it has a lot of different faces, meaning there's a lot of ways you can grasp things. Since the hand is more complicated than one would think, some types of prehension could be affected by CTS while others wil be completely fine, it all depends on which fingers need to be used and in what ways they need to be moved. Just take a look at how shifty this prehension fellow can be:

Therefore, I think it's not hard to see how prehension can be affected by CTS. For example, almost all the grasps to the left require some sort of index and middle finger flexion, as well as flexion of the thumb. Thumb opposition is also incredibly important in pinching grasps, like the Tip or 3 Jaw Chuck prehension. It's also not just the ability to perform these actions, but the amount of force and stability that can be exerted while using these grips.
Untitled illustration of prehension types
So we can speak about theoretics all day, but how has CTS affected prehension in individuals who actually have the condition? A good amount of research has been done with prehension in CTS and generally, they've found the following:
- Decreased thumb opposition range of motion (Marquardt, et al., 2014)
- Increased in digit force and net moments in whole-hand grasping (Zhang, et al., 2011)
- Increased variability with whole hand grasping and pinching (Low & Freivalds, 1999; Zhang, et al., 2011)
- Decreased ability to adjust force to object weight (i.e. using more force for heavier objects) (Zhang, et al., 2011)
The increased force might be a little surprising since we just talked about how the thumb muslces would be weakened. However, in mild to moderate CTS, the functioning of these muscles is not deteriorated to the point of not being able to exert force. The bigger issue is the lack of sensory feedback that you get from the hand. If this nasty, villainous CTS makes it harder to see what it's throwing at you, what are you going to do? Respond with full force of course! That's kind of what's happening here, when it's harder to sense if you're gripping hard enough due to lack of sensory feedback, the safer route is to use more force to make sure the object doesn't fall (remember, more force means more friction!).
So what does this mean functionally? The interesting theme that came up throughout these studies was that there were no observable differences in these prehension tasks between individuals with and without CTS. So even though those with CTS had to adjust their prehension, functionally there was no change. However, this may only be true for milder cases of CTS and not hold true if the condition continues to deteriorate.
How can an OT help?
So after all this scary talk about CTS and how it can affect your everyday functioning, seems like there’s not much hope right? Well don’t worry, here comes the last minute save from the OTs! …Okay not really. In fact, OTs would have been there all along, as they play a large role even before CTS with education and prevention, as well as being there from the start with diagnosing CTS.
Diagnosis of CTS
Diagnosis of CTS is usually done by one of two simple tests. The first is the Phalen’s test, where the client is asked to hold their forearm vertically up and let their wrist drop naturally by gravity, maintaining this position for 1 minute. If this induces numbness and tingling in the thumb, index, and middle finger, then the test would be indicative of CTS in the client.
The other tests OT easily administer is the Tinel’s test, where the OT would use an instrument to tap the median nerve in the wrist. If this elicits numbness or tingling in the same areas of the hand as the Phalen’s test, this is again indicative of CTS (East Kent Hospitals University, 2011)
Then what?
After diagnosis of CTS, the role of OT grows into providing therapy and intervention in several different way
-
Use of splinting to stabilize wrist in position that places less pressure on the carpal tunnel, also prevents the continuation of repetitive wrist movements (Mullter, et al., 2004)
-
Application of ultrasound, magnetic therapy, or low-level laser therapy (Mullter, et al., 2004)
-
Education on use of nerve gliding exercises (below) and yoga with regards to their effectiveness in treating CTS (Mullter, et al., 2004)
-
Adaptation of tools used for occupations, like a spoon or a toothbrush for ADL tasks or a writing instrument for productivity. Usually done through increased grip diameter, which requires less force to grasp on to (Trombly Latham, 2008)
-
Adaptation of the environment, especially in the office setting
-
Advocating for rest breaks and avoidance of repetitive wrist movements (De Vera Barredo & Mahon, 2007)
-
Use of ergonomic devices, especially keyboard and mouse (modified keyboard, mousepad with forearm rest to prevent wrist extension) (Doheny, Linden, & Sediak, 1995; Keir, Bach, & Rempel, 1999)
-
-
Education on task analysis, breaking down a complex task into component parts to identify steps which may exacerbate CTS (Trombly Latham, 2008)
-
For example with marking papers, it may be seen that the repetitive motion of circling mistakes with a paper can increase the risk for CTS
-
Of course these steps can be taken before CTS manifests to prevent its appearance in the first place. That way, this story of carpal tunnel syndrome can be told through someone else's eyes and not your own.
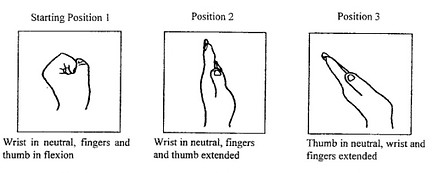
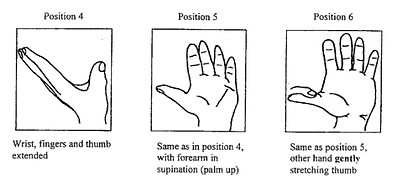
Nerve gliding
References
[Untitled illustration of prehension types]. Retrieved March 28, 2016 from http://static.memrise.com/uploads/mems/output/2379047-130622055701.png
Allman, B. (2015a). Anterior forearm & carpal tunnel. Personal Collection of Allman, B. University of Western Ontario, London, ON.
Allman, B. (2015b). Hand. Personal Collection of Allman, B. University of Western Ontario, London, ON.
Aronin, S. (2011, November). Posture, movement, and biomechanics 2- Example: Carpal tunnel syndrome. Retrieved from http://www.scottaronin.com/posture-movement-and-biomechanics-2-example-carpal-tunnel-syndrome/.
Carpal tunnel syndrome picture [Online image]. Retrieved March 28, 2016 from http://www.advancedhealthcareofthepalmbeaches.com/wp-content/uploads/2013/10/Carpal-tunnel-syndrome-picture.jpg
Children Fighting Over Toys [Online image]. Retrieved April 5, 2016 from http://d236bkdxj385sg.cloudfront.net/wp-content/uploads/mommynoire/2013/04/Children-Fighting-Over-Toys.jpg
De Vera Barredo, R., & Mahon, K. (2007). The effects of exercise and rest breaks on musculoskeletal discomfort during computer tasks: An evidence-based perspective. Journal of Physical Therapy Science, 19, 151-163.
Doheny, M., Linden, P., & Sediak, C. (1995). Reducing orthopaedic hazards of the computer work environment. Orthopaedic Nursing, 14(1), 7–15.
East Kent Hospitals University. (2011, June). Provocative tests. Retrieved from http://www.carpal-tunnel.net/diagnosing/provocative
Goss, B., & Agee, J. (2011, February). Carpal tunnel pressure- Our thoughts on its surprising dynamic behavior. Retrieved from http://www.handbiolab.com/2011/02/carpal-tunnel-pressure-our-thoughts-on-its-surprising-dynamic-behavior/.
Hand and Upper Limb Clinic. (2010). Carpal tunnel syndrome. Animated explanation [Online image]. Retrieved March 28, 2016 from https://commons.wikimedia.org/wiki/File:Carpaltunnel.gif
Keir, P. J., Bach, J. M., & Rempel, D. (1999). Effects of computer mouse design and task on carpal tunnel pressure. Ergonomics, 42(10), 1350–1360.
Lowe, B.D., Freivalds, A. (1999) Effect of carpal tunnel syndrome on grip force coordination in hand tools. Ergonomics, 42, 550–564.
Marquardt, T. L., Nataraj, R., Evans, P. J., Seltz, W. H., & Li, Z. (2014). Carpal tunnel syndrome impairs thumb opposition and circumduction motion. Clinical Orthopaedics and Related Research, 472, 2526-2533.
Mullter, M., Tsui, D., Schnurr, R., Biddulph-Deisroth, L., Hard, J., & MacDermind, J. C. (2004). Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome: A systematic review. Journal of Hand Therapy, 17, 210-228.
Nerve Gliding [Online image]. Retrieved April 5, 2016 from http://www.carpal-tunnel-symptoms.com/images/2nerveglide-bigger.jpg
Palmer, K. T., Harris, E. C., & Coggon, D. (2007). Carpal tunnel syndrome and its relation to occupation: A systematic literature review. Occupational Medicine, 57, 57-66.
Spaulding, S. J. (1988). The biomechanics of prehension. American Journal of Occupational Therapy, 43(5), 302-307.
Spinning quarter [Online image]. Retrieved April 5, 2016 from https://newhopeinternationalministries.files.wordpress.com/2013/07/spinning-quarter.jpg
TeachMeAnatomy. Palmer view of the thenar muscles of thumb and hand [Online image]. Retrieved April 5, 2016 from http://teachmeanatomy.info/wp-content/uploads/Palmar-View-of-the-Thenar-Muscles-of-the-Thumb-and-Hand-Labelled-TeachMeAnatomy.jpg
Thomsen, J. F., Gerr, F., & Atroshi, I. (2008). Carpal tunnel syndrome and the use of computer mouse and keyboard: A systematic review. BMC Musculoskeletal Disorders, 9(134), doi:10.1186/1471-2474-9-134.
Trombly Latham, C. A. (2008). Occupation as therapy: selection, gradation, analysis, and adaptation. In Radomski, M. V., Trombly Latham, C. A. Occupational therapy for physical dysfunction (6th ed.). Philadelphia: Lippincott Williams and Wilkins
Zachary, T. [doczac]. (2008, May 14). Grip strength & hand exercise. [Video file]. Retrieved from https://www.youtube.com/watch?v=i6j6jUFKQNA
Zhang, W., Jonston, J. A., Ross, M. A., Smith, A. A., Coakley, B. J., Gleason, E. A., Dueck, A. C., & Santello, M. (2011). Effects of carpal tunnel syndrome on adaptation of multi-digit forces to object weight for whole-hand manipulation. PLoS ONE, 6(11), doi:10.1371/journal.pone.0027715.